")
Coding Edge
Improving documentation techniques
By James Collins, M.D.
Reconstructive Surgeon
Documentation is an important part of every patient encounter. Documentation can ensure that the care provided to a patient is accurately conveyed to other healthcare providers, patients, and payors. The BRCA policy is that all documentation is to be completed in a timely manner within 14 days of rendering care to a patient. Errors, inaccuracies, and poorly written notes can result in medical errors, delay of care, and loss of revenue even when documentation is completed in a timely manner. The purpose of this article is to describe why poor documentation may result in these types of errors, and how our providers might implement habits that will reduce the frequency and impact of these errors. The article will focus primarily on operative summaries, but the same habits apply to all phases of care.
Our practice includes multiple facilities with providers traveling to different locations and billing offices that are often located at distant sites. When care is transferred from one provider to another, documentation often provides the best and most efficient manner to ensure a good and consistent treatment plan is maintained for that patient. Documentation should be concise, specific, easily read, and helpful.
During my time as a physician located in Augusta, GA, at our corporate office, I read many of the notes from our physicians and extenders. I did this both as a physician taking over care from other providers and as a physician assisting the billing office to decipher some of our operative summaries. Using this experience, I drafted the following representative operative summary to serve as a bad example:
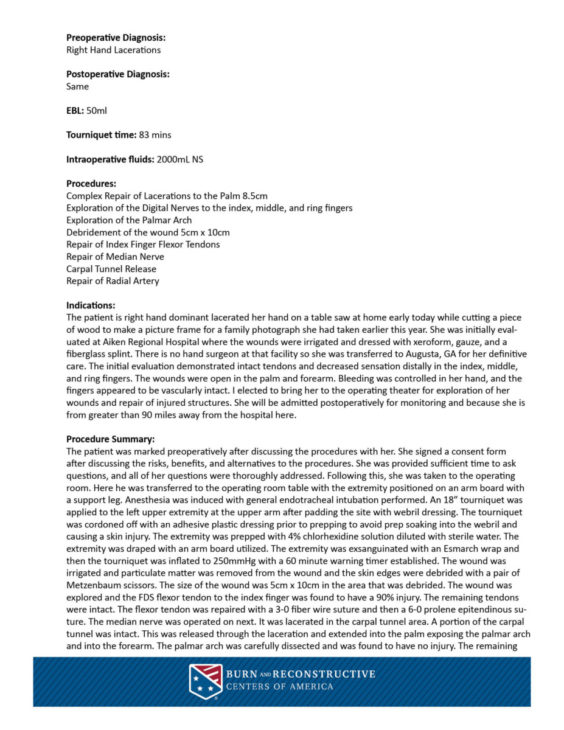

If you took the time to try to read through the operative summary, thank you. I know you likely did not enjoy it. It should not matter if you are a hand surgeon, burn surgeon, hospitalist, physician’s assistant, nurse, or janitor. This is a bad note. It is difficult for all of us to read, and therefore it is difficult to provide care for the patient.
I see these types of notes often, and they are very difficult to read. I have a hard time figuring out what was done in the operation. The notes require a significant amount of time to read through. Even with ample time to read the bad example note above, I would have a difficult time figuring out what the appropriate care plan is for the patient or what the appropriate billing codes are for the patient.
Documentation can be poor for multiple reasons including wordiness, formatting, oversimplification, and factual errors. Each of these things contributes in some way and will be addressed using examples from the note above. In the following sections, I will take the operative summary and correct them until we have an easy to read note.
Wordiness
I must admit that I am a logophile and wanted to label this category “loquaciousness” or “prolixity”, but it would be inappropriate as an author tasked with sharing information. Using as few words as possible to describe what is happening is important because the reader can focus on important things. If we run a word count on the operative summary of the “bad example”, we find there are 626 words in the section and 174 words before we even start the procedure. Considering that the average reading speed is around 300 words per minute, it takes 30 seconds to even get to the start of the procedure and more than two minutes to read the note.
Wordiness can come from a desire to be very specific about details of an operation to avoid lawsuit or to justify a procedure. This can be compounded when the author of the note does not fully understand why they are writing the words that they are. Every expert I have read or learned from on this topic has stated that concise and simple documentation is safer from litigation. I would add that if you are confused when you are wording your documentation, the reader of your note will not be less confused than you.
Using the principles of simplification and removing unnecessary language, our procedure summary would be reduced to 337 words and read like this:
After the patient was marked and informed consent was received, the patient was brought to the operating room where anesthesia was induced, and she was prepped and draped. A padded tourniquet was applied to the left upper extremity prior to prepping. The extremity was exsanguinated with an Esmarch wrap, and the tourniquet was inflated to 250mmHg with a 60-minute timer. The wound was irrigated, and particulate matter was removed from the wound and the skin edges were sharply debrided. The size of the wound was 5cm x 10cm at the distal forearm/wrist. The wound was explored and the FDS flexor tendon to the index finger was found to have a 90% injury. The remaining tendons were intact. The flexor tendon was repaired with a 3-0 fiber wire suture and then a 6-0 prolene epitendinous suture. The median nerve was completely transected in the carpal tunnel. The intact portion of the carpal tunnel was released for exposure and the lacerations were extended proximally and distally. The palmar arch was noted to be intact without injury, as were the proper digital nerves. The median nerve was directly repaired under loupe magnification with 8-0 nylon epineurial sutures after sharply excising the nerve ends to healthy fascicles and aligning the fascicles/extraneural landmarks. The radial artery was noted to be lacerated. This was repaired after dissecting the artery ends and preparing them under loupe magnification. The vessels were flushed with the tourniquet down to confirm arterial flow. The artery ends were coapted with 8-0 nylon interrupted sutures. The vessel was irrigated with 4% lidocaine for vasodilation following the repair and confirmation of anterograde blood flow across the anastamosis. The wounds were closed with 3-0 prolene horizontal mattress sutures measuring 8.5cm in total length. The PA/NP worked simultaneously with me, reducing the time spent to complete the procedure. If the PA had not been present, then I would have been required to spend a longer time in the operating room and resulted in increased hospital cost associated with the facility and anesthetic.
Formatting
When considering formatting, most of our providers consider the section headings but often because of dictation systems completely ignore punctuation and creating paragraphs. This can lead to run-on sentences and large blocks of text with too much information to identify the important parts. Compare the less wordy version of the procedure summary above with the one below. All that has been done is breaking it into paragraphs based on what part of the procedure is being performed.
After the patient was marked and informed consent was received, the patient was brought to the operating room where anesthesia was induced, and she was prepped and draped. A padded tourniquet was applied to the left upper extremity prior to prepping. The extremity was exsanguinated with an Esmarch wrap, and the tourniquet was inflated to 250mmHg with a 60-minute timer.
The wound was irrigated, and particulate matter was removed from the wound and the skin edges were sharply debrided. The size of the wound was 5cm x 10cm at the distal forearm/wrist.
The wound was explored and the FDS flexor tendon to the index finger was found to have a 90% injury. The remaining tendons were intact. The flexor tendon was repaired with a 3-0 fiber wire suture and then a 6-0 prolene epitendinous suture.
The median nerve was completely transected in the carpal tunnel. The intact portion of the carpal tunnel was released for exposure and the lacerations were extended proximally and distally. The palmar arch was noted to be intact without injury, as were the proper digital nerves. The median nerve was directly repaired under loupe magnification with 8-0 nylon epineurial sutures after sharply excising the nerve ends to healthy fascicles and aligning the fascicles/extraneural landmarks.
The radial artery was noted to be lacerated. This was repaired after dissecting the artery ends and preparing them under loupe magnification. The vessels were flushed with the tourniquet down to confirm arterial flow. The artery ends were coapted with 8-0 nylon interrupted sutures. The vessel was irrigated with 4% lidocaine for vasodilation following the repair and confirmation of anterograde blood flow across the anastamosis.
The wounds were closed with 3-0 prolene horizontal mattress sutures measuring 8.5cm in total length.
The PA/NP worked simultaneously with me, reducing the time spent to complete the procedure. If the PA had not been present, then I would have been required to spend a longer time in the operating room and resulted in increased hospital cost associated with the facility and anesthetic.
Now each portion of the procedure is separated into its own paragraph. There is a tendon paragraph, a nerve paragraph, and an artery paragraph. If I want to know what type of tendon repair was done in follow up, I have an easier time finding that section.
Oversimplification
Oversimplification means leaving out information important for decision making past and future. With the example treated for wordiness and formatted into sections, it is easier to find the missing pieces of information in the example.
Because most of my practice is hand surgery, I used this as an example. I know many of our practitioners are not hand surgeons, so I will provide additional background for this example. Flexor tendon lacerations greater than 50% of the cross-sectional area of the tendon require suture repair, splinting, and immediate active therapy when possible to achieve the best outcomes. Ability to begin therapy immediately is determined by the type of repair. In our example, the type of repair was not described nor was the type of splint placed at the end of the procedure.
The wound was explored and the FDS flexor tendon to the index finger was found to have a 90% injury. The remaining tendons were intact. The flexor tendon was repaired with a 3-0 fiber wire four core stranded cruciate repair and then a 6-0 prolene epitendinous suture.
…
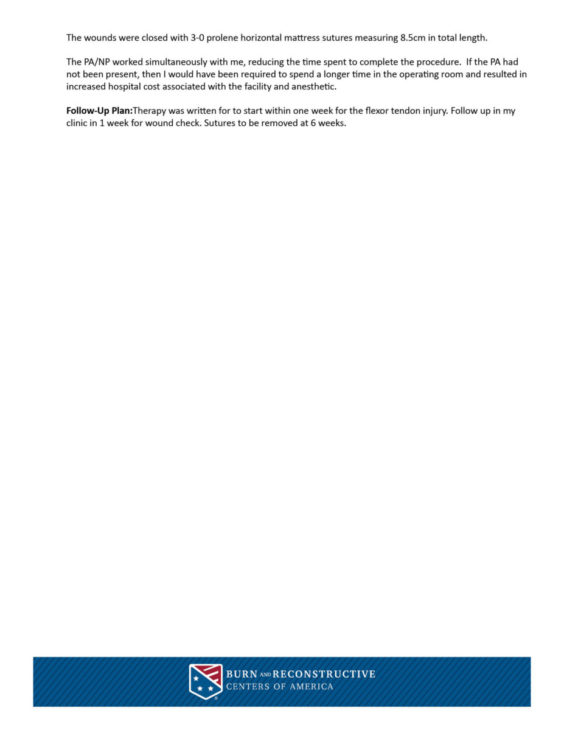
The wounds were closed with 3-0 prolene horizontal mattress sutures measuring 8.5cm in total length. The wounds were dressed with ointment, xeroform, gauze, webril, and a dorsal blocking plaster short arm splint.
The PA/NP worked simultaneously with me, reducing the time spent to complete the procedure. If the PA had not been present, then I would have been required to spend a longer time in the operating room and resulted in increased hospital cost associated with the facility and anesthetic.
Applying These to the Entire Document
In this section, I wanted to apply what I have described to the entire operative summary including the initial headings. The order of the sections was confusing. The diagnosis sections are oversimplified, the procedures performed listed include some questionable unbundling, and the indications section is verbose and poorly formatted. Here's the revised version:
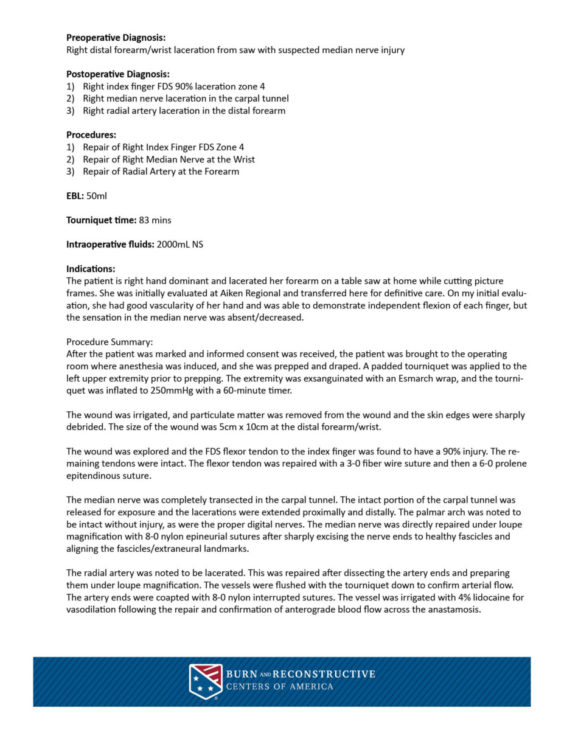
At the very end of this operative summary, note that I added the “Follow-Up Plan” section. The section describes a clear and easy to read section that shares our plans for the patient. I honestly believe that anyone with a modest amount of medical training would be able to describe what happened to this patient and what the plan was after reading the note for less than two minutes.
Factual Errors
These types of errors are sometimes the hardest to address because they are often inadvertent. They can be caused by an error in knowledge, but also by a missed keystroke or a misspoken word. They cannot always be avoided, but if a note is easy to read, it is more likely to be caught. Can you identify the error in the note above?
I purposefully included the error of listing the left hand in the procedure summary body and the right hand in the procedures performed. Having an easy-to-read note makes it easier to find this type of error. Some errors might not make a difference in future care, but others are not so benign.